

You’ve been told to rest, but nobody’s given you a straight answer on when you’ll actually be back on your feet. That’s the frustrating part of a foot stress fracture: the pain is often manageable, yet the timeline feels like a moving target. If you’re searching for stress fracture foot recovery time, you want real numbers, not vague reassurance.
Most stress fractures in the foot take between six and eight weeks to heal, though this shifts depending on the bone involved, how early you caught it, and how strictly you follow activity restrictions. A fracture in the fifth metatarsal or navicular bone can take considerably longer than one in a lesser metatarsal, and returning to sport too soon is the single biggest reason recovery drags on past the expected window.
In this guide, we’ll walk through what actually happens during each stage of healing, from the first weeks in a boot or cast through to graduated return to activity. We’ll cover how immobilisation speeds things along, what slows it down, and when it’s time to see a podiatrist rather than wait it out at home.
Why stress fracture recovery time varies so much
Ask five different patients how long their stress fracture took to heal, and you’ll get five different answers. That’s not because anyone did anything wrong. Bone location, how quickly the fracture was diagnosed, and your own bone health all play a part, and any one of them can add weeks to the process. Understanding why the timeline shifts helps you stop comparing your recovery to someone else’s Instagram post about their marathon comeback.
The bone involved changes everything
Not all foot bones heal at the same speed, and this is the single biggest factor behind the wide range you’ll see quoted online. The metatarsals (the long bones behind your toes) generally have a good blood supply and heal within six to eight weeks if you stick to the plan. The navicular bone and the base of the fifth metatarsal are a different story. Both sit in areas with a comparatively poor blood supply, which means bone-forming cells take longer to do their job.

A stress fracture in the navicular or fifth metatarsal can take twice as long to heal as one in a lesser metatarsal, simply because of where it sits in the foot.
| Bone location | Typical healing time | Risk profile |
|---|---|---|
| 2nd, 3rd, 4th metatarsal shaft | 6-8 weeks | Lower risk |
| 1st metatarsal | 6-8 weeks | Lower risk |
| 5th metatarsal (base) | 8-12+ weeks | Higher risk |
| Navicular | 12-16+ weeks | Higher risk |
| Calcaneus (heel bone) | 8-10 weeks | Moderate risk |
These figures assume you follow your treatment plan properly. Skip the boot for a big night out or go back to running early, and even a low-risk fracture can turn into a stubborn, slow-healing one.
How early you were diagnosed matters
Catching a stress fracture early gives you a significant advantage, because early-stage bone stress reactions haven’t yet progressed to a full break in the bone. Delayed diagnosis is one of the most common reasons recovery drags out longer than it should. Many people push through weeks of nagging foot pain before getting it checked, often because the pain fades with rest and returns with activity, a classic stress fracture pattern that’s easy to dismiss as "just sore feet."
By the time you’re finally scanned, the fracture may have worsened from a hairline stress reaction into a displaced or more advanced injury, which needs longer immobilisation and sometimes a different treatment approach altogether. If you’ve had foot pain that worsens with weight-bearing activity and doesn’t settle within a week or two of reduced activity, don’t wait it out. Get it imaged.
Age, bone density and general health
Your body’s baseline bone health has a direct bearing on how fast new bone forms. Bone density naturally declines with age, and conditions like osteoporosis or osteopenia slow the mineralisation process that stress fractures rely on to heal. According to Healthdirect Australia, low bone density is a recognised risk factor for stress fractures generally, not just a coincidence found in older patients.
Other factors that quietly extend recovery include:
- Nutritional deficiencies, particularly low calcium, vitamin D, or overall calorie intake (common in athletes under-fuelling for training load)
- Smoking, which restricts blood flow to healing tissue and is well documented as slowing fracture repair
- Hormonal factors, including menstrual irregularities in female athletes, which can affect bone density
- Diabetes or other conditions that affect circulation and healing capacity
- Previous stress fractures, which suggest an underlying biomechanical or training issue that needs addressing, not just this one injury
How strictly you follow activity restrictions
Here’s the factor that’s actually within your control: compliance. Podiatrists see this pattern constantly. Two patients with the same fracture in the same bone, treated with the same protocol, end up with wildly different recovery times because one followed the immobilisation instructions and the other didn’t. Weight-bearing too early, even just walking around the house without the boot, reloads the bone before the repair process has laid down enough new tissue to handle the stress.
Recovery isn’t just about waiting out a calendar. It’s about giving damaged bone the mechanical rest it needs to rebuild properly. Every time you cheat the boot or skip a rest day because "it doesn’t hurt much," you’re resetting part of that repair process, sometimes without even feeling it happen until the pain flares up again a few days later.
How to support your stress fracture recovery
While the bone itself does the actual healing, what you do around that process makes a measurable difference to your timeline. Immobilisation devices, nutrition, and how you manage pain all influence whether you hit the six-week mark or drift towards the twelve-week end of the range. None of this is complicated, but it does require consistency.
Get the right immobilisation device early
A CAM walking boot is the standard first-line treatment for most foot stress fractures, and it works by taking load off the injured bone while still letting you get around. For higher-risk fractures, such as the navicular or fifth metatarsal base, a podiatrist may recommend a non-weight-bearing period with crutches before you progress to a boot. Skipping this step, or swapping to normal shoes the moment the pain eases, is one of the most common reasons a straightforward fracture turns into a drawn-out one.

The boot isn’t a suggestion, it’s the treatment. Wearing it properly for the full prescribed period is what actually shortens your recovery.
Most patients wear a boot for four to eight weeks depending on the bone involved, then move to a supportive shoe with a stiff-soled insert for a transition period before returning to normal footwear.
Fuel the bone-building process
Bone repair is metabolically demanding, and under-fuelling slows it down. Calcium and vitamin D are the obvious nutrients, but adequate overall energy intake matters just as much, particularly for athletes who cut calories while injured because they’re moving less. Talk to your GP or a sports dietitian if you’re unsure whether your diet is supporting healing rather than working against it.
- Calcium-rich foods: dairy, leafy greens, tinned fish with bones
- Vitamin D: sensible sun exposure, oily fish, fortified foods, or a supplement if levels are low
- Adequate protein: needed for the collagen matrix that new bone is built on
- Sufficient total calories: don’t use the injury as a reason to under-eat
Manage pain without ignoring what it’s telling you
Over-the-counter pain relief can help you get through the day, but it shouldn’t become a reason to push activity further than your podiatrist has cleared. Some evidence suggests that regular high-dose NSAID use may interfere with bone healing, so it’s worth checking with your GP or pharmacist about which pain relief options are appropriate while a fracture heals, rather than defaulting to whatever’s in the cabinet.
Swelling and discomfort that flare up after you’ve been more active than planned are a signal, not something to medicate through and ignore. Treat pain as useful feedback throughout your recovery, not an obstacle to override.
Keep moving the parts that aren’t injured
Understandably, most people go completely sedentary once they’re in a boot, but this isn’t necessary and can slow your broader recovery from a fitness standpoint. Upper body strength work, seated core exercises, and swimming with a waterproof boot cover (once cleared by your podiatrist) all keep you conditioned without loading the healing bone. Staying active elsewhere also helps with the mental side of a long recovery, which matters more than most people expect when weeks of restricted movement stretch ahead.
What to expect week by week during recovery
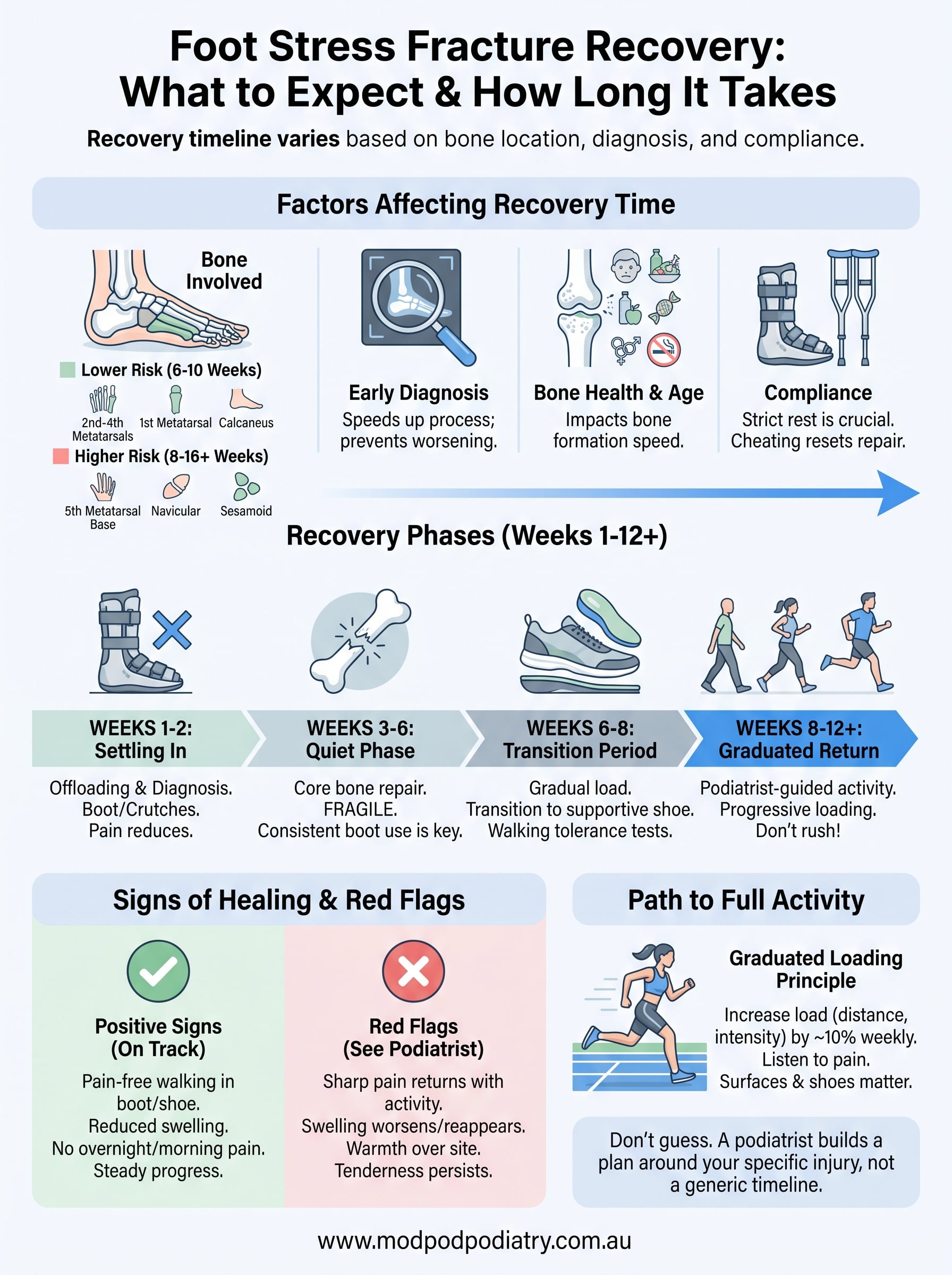
Knowing the average healing time is useful, but it doesn’t tell you what actually happens during those weeks. Foot stress fracture recovery moves through fairly predictable phases, even though the exact length of each phase depends on the bone involved and how well you stick to the plan. Here’s a realistic breakdown of what most patients go through, from diagnosis to full activity.
Weeks 1 to 2: settling in
Just after diagnosis, the priority is getting the bone completely offloaded. You’ll usually be fitted with a CAM boot, sometimes alongside crutches for a few days if weight-bearing is still painful. Pain often improves quickly once the boot is on and load is removed, which can be misleading. Feeling better doesn’t mean the bone has healed; it means the aggravating force has stopped. Most people also have a short review appointment in this window to confirm the diagnosis with imaging and rule out anything more serious.

Weeks 3 to 6: the quiet phase
This stretch is where most of the actual bone repair happens, and it’s also where compliance tends to slip because things feel fine. You’re walking in the boot, daily life has mostly returned to normal, and the temptation to test the foot without it grows. Resist it. This is the phase where new bone formation is at its most fragile, and reloading too early undoes weeks of progress.
The bone looks and feels stable long before it’s actually strong enough to handle full load again.
Most podiatrists will schedule a check-in around the six-week mark to assess pain levels, tenderness on palpation, and sometimes repeat imaging for higher-risk fractures like the navicular or fifth metatarsal.
Weeks 6 to 8: the transition period
Once your podiatrist confirms the fracture is healing on schedule, you’ll typically move out of the boot and into a supportive shoe with a stiff-soled insert or orthotic. This isn’t the finish line, it’s a gradual handover of load back onto the bone. Walking tolerance is tested first, short distances on flat ground, before anything resembling exercise gets introduced. Any return of sharp, localised pain at this stage is a signal to slow down, not push through.
Weeks 8 to 12+: graduated loading
For lower-risk metatarsal fractures, this is often when structured return-to-activity begins, following a plan your podiatrist builds around your sport or daily demands. For higher-risk fractures such as the navicular or fifth metatarsal base, this phase might still involve continued protection and a slower reintroduction of load, sometimes with repeat scans to confirm bone healing before running or jumping is cleared.
| Weeks | What’s happening | What you should be doing |
|---|---|---|
| 1-2 | Diagnosis confirmed, load removed | Boot or crutches, full compliance |
| 3-6 | Core bone repair | Boot worn consistently, no shortcuts |
| 6-8 | Bone strengthening, load transition | Supportive shoe, walking tolerance tests |
| 8-12+ | Graduated return to activity | Podiatrist-guided loading program |
Setbacks happen, and they’re usually a sign that one phase was rushed rather than a random bad break. If pain returns after you’ve progressed a stage, it’s worth stepping back to the previous phase rather than pushing through and hoping it settles on its own.
Recovery times for different types of foot stress fractures
Grouping stress fractures by location gives you a far more accurate timeline than a single blanket number, because where the fracture sits changes everything about how it heals. Metatarsal fractures make up the majority of cases podiatrists see, while fractures in the navicular, fifth metatarsal base, calcaneus and sesamoid bones each follow their own healing pattern and carry a different risk of complication. Matching your fracture against the right category below is the fastest way to set a realistic expectation for how many weeks you’re actually looking at.
Metatarsal shaft fractures (the most common type)
Second, third and fourth metatarsal shaft fractures are diagnosed more often than any other foot stress fracture, largely because these bones absorb repetitive load every time you run, jump or push off. Healing typically takes six to eight weeks in a CAM boot, with graduated return to activity starting around week six for uncomplicated cases. First metatarsal fractures follow a similar timeline, though they’re less common overall because this bone is thicker and better supported by surrounding structures.
Fifth metatarsal base fractures
Fractures at the base of the fifth metatarsal, sometimes classified as Jones fractures depending on the exact zone, heal more slowly because blood supply to this part of the foot is comparatively poor. Recovery generally runs eight to twelve weeks, and a meaningful number of cases don’t heal fully with immobilisation alone. The Better Health Channel notes that fractures in poorly vascularised bone can require longer management, and in this specific case that sometimes means surgical fixation with a screw, particularly for athletes who need a faster, more reliable return to sport.
Navicular stress fractures
Navicular fractures are notorious among podiatrists for being slow and stubborn, sitting as they do in a low blood supply zone in the middle of the foot’s arch. Recovery often takes twelve to sixteen weeks or longer, frequently starting with a period of complete non-weight-bearing before any boot use even begins. Overlooking early navicular symptoms, or continuing to train through vague, hard-to-pin-down arch pain, is one of the most common reasons this particular bone ends up needing surgery instead of straightforward immobilisation.

Navicular and fifth metatarsal fractures are the two most likely to need surgical input if immobilisation alone doesn’t work, so early diagnosis matters more here than anywhere else in the foot.
Calcaneal and sesamoid fractures
Calcaneal, or heel bone, stress fractures typically heal within eight to ten weeks, and because the heel bears weight but has a reasonable blood supply, straightforward immobilisation usually does the job. Sesamoid fractures, the small bones tucked under the big toe joint, present a different challenge entirely: they heal slowly, often over ten to twelve weeks, partly due to a naturally limited blood supply and partly because they’re genuinely difficult to fully offload, even inside a boot.
| Fracture type | Typical recovery | Non-weight-bearing phase needed? | Surgical risk |
|---|---|---|---|
| Metatarsal shaft (2nd-4th) | 6-8 weeks | Rarely | Low |
| 1st metatarsal | 6-8 weeks | Rarely | Low |
| 5th metatarsal base | 8-12 weeks | Sometimes | Moderate |
| Navicular | 12-16+ weeks | Often, early on | Higher |
| Calcaneus | 8-10 weeks | Rarely | Low |
| Sesamoid | 10-12 weeks | Sometimes | Low-moderate |
Understanding which category your fracture falls into won’t change the biology of how it heals, but it will change how you plan the weeks ahead, from work commitments to when you can realistically talk to your podiatrist about lacing up for training again.
Signs your stress fracture is healing well or not
Guessing how your foot is doing based on how it feels day to day is unreliable, because pain isn’t a perfectly accurate gauge of bone healing. Some fractures feel almost normal well before the bone is strong enough to handle full load, while others ache on and off for weeks after the repair is well underway. Knowing the actual markers of healing, rather than just tracking pain, helps you avoid both extremes: pushing too early or staying overly cautious long after you could have progressed.
Positive signs your recovery is on track
Watching for these signs across the weeks gives you a clearer picture than a single good or bad day ever will:
- Pain-free walking in the boot or supportive shoe, with no tenderness when your podiatrist presses directly on the fracture site
- Reduced swelling around the injured area, particularly noticeable by the end of the day
- No pain overnight or first thing in the morning, which often lingers longest in fractures that are still actively inflamed
- Steady progress through each phase without needing to step back to an earlier stage
- Confirmed healing on imaging, where repeat X-rays or scans are used for higher-risk fractures like the navicular or fifth metatarsal base
If you’re ticking most of these boxes by the timeline your podiatrist gave you, you’re in good shape to progress to the next phase of loading.
Red flags that need a podiatrist’s attention
Certain symptoms mean something isn’t healing the way it should, and waiting them out rarely helps. Localised, sharp pain that returns with weight-bearing after a period of feeling fine is the clearest warning sign, because it usually means the bone has been reloaded before it was ready. Swelling that reappears or worsens, particularly alongside warmth over the fracture site, also deserves a proper look rather than a wait-and-see approach.
If pain that had settled comes back once you increase activity, that’s the bone telling you it isn’t ready, not a sign to push through.
Other signs worth flagging to your podiatrist include pain that spreads beyond the original site, a limp that develops or worsens over time, or tenderness that hasn’t budged despite weeks in a boot. According to Healthdirect Australia, persistent or worsening pain after a fracture diagnosis is one of the clearest indicators that a treatment plan needs reassessing, and it shouldn’t be ignored in the hope it resolves on its own.
When pain returns after progress
Setbacks midway through recovery are common, and they don’t automatically mean something has gone seriously wrong. Often it simply means one phase was progressed a little too quickly, and stepping back to the previous stage, whether that’s more time in the boot or a return to non-weight-bearing, gives the bone the chance to catch up. Tracking your symptoms against the table below helps you decide whether what you’re feeling is normal transition soreness or something that needs a review.
| Symptom pattern | Likely meaning | What to do |
|---|---|---|
| Dull ache easing within a day of increased activity | Normal loading response | Continue as planned |
| Sharp pain at the fracture site, doesn’t ease with rest | Bone stress reaction returning | Step back a phase, contact podiatrist |
| Swelling that builds through the day | Tissue still adjusting | Monitor, ice if needed |
| Swelling with warmth and worsening pain | Possible re-injury or delayed healing | See your podiatrist promptly |
Acting on these signals early, rather than hoping they settle by themselves, is what keeps a minor setback from turning into a much longer recovery.
How to return to sport and exercise safely
Getting the all-clear to start moving again feels like the finish line, but this is actually where a lot of recoveries go wrong. Returning to sport too quickly after a foot stress fracture is the single most common cause of re-injury, and it’s almost always driven by impatience rather than bad luck. The bone might look healed on a scan and feel strong on a short walk, yet still lack the fatigue resistance needed to handle repeated impact from running, jumping or changing direction.
The graduated loading principle
Bone adapts to load gradually, so your return needs to follow the same logic, building tolerance in small, deliberate steps rather than jumping straight back into training. Podiatrists typically use a graduated loading program that increases distance, intensity or impact by no more than about 10% each week, checking in regularly to make sure pain and swelling stay absent. Skipping stages because "it feels fine" is exactly how a manageable six-week recovery turns into a three-month setback.
Bone needs progressive load to get strong again, not a single test run to prove it’s ready.
A sample return-to-run progression
Every return plan should be built around your specific fracture, sport and fitness level, but a typical progression for a lower-risk metatarsal fracture might look like this:
- Week 1: Walking without pain in normal shoes, no boot required
- Week 2: Brisk walking and light stationary cycling, no impact
- Week 3: Walk-jog intervals on flat, even ground (for example, 1 minute jog, 2 minutes walk)
- Week 4: Continuous light jogging, gradually extending duration
- Week 5-6: Introduce easy running on varied terrain, still avoiding hard surfaces
- Week 7+: Sport-specific drills, sprinting, jumping and cutting, only once running is fully pain-free
Higher-risk fractures such as the navicular or fifth metatarsal base often need a slower version of this same sequence, with extra checkpoints from your podiatrist before each stage.
Warning signs during return to activity
Progressing through any of these stages should never come at the cost of pain. If discomfort appears during or after a session, that’s a clear signal to repeat the previous stage rather than push forward and hope it settles. Pain that shows up the next morning, rather than during the activity itself, is just as meaningful and often gets ignored because it’s easy to blame on general soreness instead of the healing bone.
Other things worth flagging to your podiatrist during this phase include a change in your running gait, favouring one side, or swelling that builds after sessions rather than easing off within a few hours. According to the Australian Institute of Sport, gradual load management is one of the most effective strategies for preventing bone stress injuries from recurring in athletes, and the same principle applies just as strongly on the way back from an existing fracture as it does in preventing the first one.
Surfaces matter too. Trading concrete for grass or a synthetic track in the early weeks reduces impact loading substantially, giving the bone one less variable to cope with while it finishes remodelling. Footwear should also be reviewed at this stage, since worn-out or unsupportive shoes can undo weeks of careful progress by reintroducing exactly the kind of repetitive stress that caused the fracture in the first place.
Your path back to full activity
Stress fracture recovery isn’t a single number you can pin down before you’ve even been scanned. It’s a process shaped by which bone broke, how early you caught it, and how honestly you stuck to the boot when nobody was watching. Six to eight weeks covers most metatarsal fractures, but navicular and fifth metatarsal injuries can push well past three months, and rushing either one almost always costs you more time than it saves.
What actually shortens your timeline is boring, consistent compliance: wearing the boot properly, fuelling the bone, and progressing load in small steps rather than one hopeful test run. If your foot pain hasn’t settled, or you’re not sure which phase you’re actually in, don’t guess your way through it. A podiatrist can confirm exactly where you stand and build a plan around your bone, not a generic timeline. Book online with ModPod Podiatry and get a clear answer instead of another week of uncertainty.

